
Some facts to help you tune up your BS Detector.
Introduction
This story is about the harm that can come when officials provide false assurances, stated with great certainty, about scary things.
The current example is monkeypox. The disease is spreading, and so are the misleading messages from press and health officials about its potential danger.
It could be that they are well-intentioned people trying to prevent panic. After all, we have the means to prevent, treat, and contain this disease. But if they are not more candid, the public may not understand that there is, in fact, something scary to contain.
And, occasionally, something more than cynicism can be discerned behind these false public assurances: a campaign of deliberate deception for political or economical reasons. An extreme example of this is the official response to the poisonous air resulting from the attack on the World Trade Center on 9/11. As detailed below, beyond the 3,000 people killed in the attack, many thousands more were harmed by the deceptive statements issued in the days following — and those tragic losses could have been reduced had officials been transparently honest about what was happening.
Now we have no reason to believe that anything sinister is behind the misleading public pronouncements about monkeypox. But now is the time to carefully evaluate anything you hear or read about the disease — and to be on the alert for any message that seems to be promoting a particular agenda rather than sticking closely to the known facts.
Here’s a brief guide to help you do just that.
Monkeypox Is Spreading
Monkeypox continues to spread. The World Health Organization (WHO) announced that as of May 31, there are now more than 550 cases in 30 countries. An official at the WHO said, “We’re seeing cases all appearing in a relatively short period of time. …This is different. This has not been seen before.” (Add one more: Yesterday, June 1, a man from Georgia with a “history of international travel” was reported to have been infected.)
Yet, for over a month now, many in the media have been pooh-poohing the potential dangers of monkeypox, downplaying its symptoms and its infectiousness, and misrepresenting the ways it can be transmitted. And they suggest that only gay people should be worried.
This kind of talk makes me nervous. Even if all of it turns out to be correct, what bothers me is the speakers’ inappropriate certainty on matters not yet understood.
People have died because they believed unproven public declarations — stated with great confidence — by officials who should have known better. In some cases, the talking heads did know better but, for political or economic reasons, promoted a lie.
The story of COVID-19 is a spectacular example. It was first presented as no more serious than a cold, and masks were first presented as ineffective. Now face coverings are considered vital.
‘Conscience-Shocking’ Misleading Statements
Here is a more sharply defined example of how deadly the appearance of absolute certainty can be. In this case, it was for cynical reasons.
After the 9/11 attack on the World Trade Center, downtown New York remained contaminated with clouds of toxic dust and debris, full of asbestos, lead, mercury, glass, organic pollutants (dead people), byproducts of fuel combustion, and so on. Yet, within days of the attack, Christine Todd Whitman, then administrator of the Environmental Protection Agency, announced, with great certainty, that the “air is safe to breathe” — long before tests had been completed.
Later, sick and dying victims of this deception tried to sue her. In 2006, a Manhattan Federal District Court judge declined to dismiss charges against Whitman, saying she “made statements about safety that were so misleading that they were ‘conscience-shocking.’” But, two years later, a federal appeals court judge dismissed the lawsuit. His rationale is revealing:
Mrs. Whitman … was forced to balance competing interests after the attack. The court found that complying with instructions from the White House to hasten the return of financial workers to Wall Street as soon as possible after the World Trade Center was destroyed conflicted with Mrs. Whitman’s obligation to highlight the health risks facing people who lived, worked or went to school in Lower Manhattan.
In other words, she was only “following orders” when she chose to put hundreds of emergency workers at risk. (To learn more about the role of the Bush White House in this deception, go here.)
Those most affected were the men — most of whom were not wearing respiratory equipment — who worked directly in the smoking remains of the World Trade Center.
I personally witnessed then-Mayor Rudy Giuliani’s macho strutting around the site without a respirator, setting a manly example for the men forced to work long hours lest they be fired. (The New York Times published a sanitized account of Giuliani’s behavior.)
As of 2018, nearly 10,000 first responders and others who were in the World Trade Center area on 9/11 had been diagnosed with cancer. More than 2,000 deaths were attributed to 9/11 illnesses. Many others developed chronic respiratory diseases, such as COPD.
Getting Back to Monkeypox
It isn’t just cable pundits who have been downplaying and misrepresenting the disease. Official sources are also guilty. One particular idea they promote, perhaps inadvertently, creates the impression that a mask would not protect you under any circumstances. They say you can only get the disease with prolonged body contact, and they imply that there is no danger of inhaling it.
At the World Economic Forum in Davos, Switzerland, Richard Hatchett, the CEO of CEPI (Coalition for Epidemic Preparedness Innovations), told CNBC:
Monkeypox is a very different disease than COVID. It does not spread through respiratory transmission in the same way, so it does not present the kind of global threat that many of us immediately recognized that COVID presented.
But experts say that monkeypox can be transmitted via respiratory droplets at close range. These large droplets are not the same as aerosolized virus particles that can travel over longer distances the way COVID-19 can — but they are infectious.
And, because the symptoms of monkeypox include sore throat and coughing, infected people can be spreading those droplets.
You can avoid intimate body contact with an infected stranger sitting or standing next to you — but you may not be able to avoid inhaling their respiratory droplets, which is why, in many situations, wearing a mask seems like a good idea.
Two Kinds of Monkeypox
There are two kinds, or “clades,” of monkeypox, one worse than the other. So far, the reported current cases in Europe and the US are, presumably, the milder form (endemic especially to Nigeria and Cameroon) with a death rate of 3.6 percent. But even this kind is dangerous for children, the elderly, and the immunocompromised.
Monkeypox from the Congo Basin is more virulent, with a death rate of 10.6 percent. Worse yet, it is more transmissible from human to human.
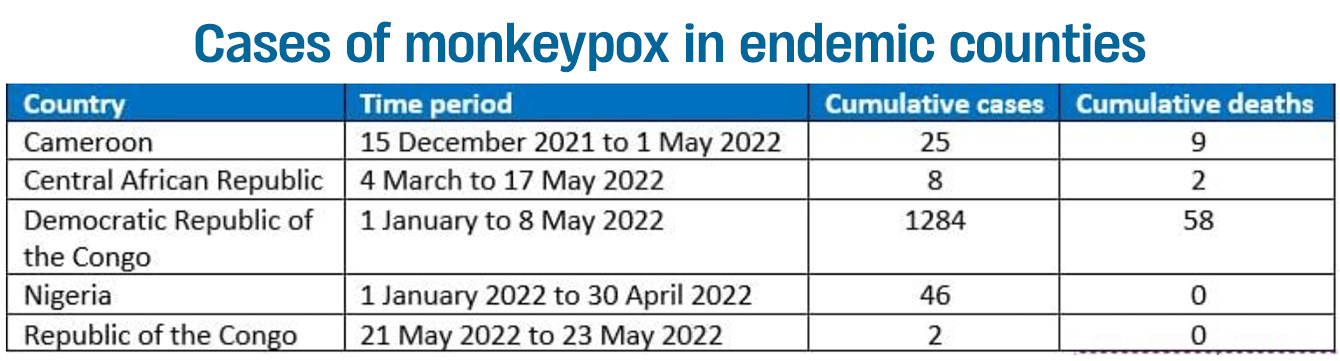
Between January 1 and May 22, the Democratic Republic of the Congo had 1,284 new cases, with 58 deaths — according to the World Health Organization.
Curiously, these figures are contradicted by a health official in the Congo who was quoted by the Associated Press and Washington Post. Dr. Aime Alongo, chief of the Sankuru health division in Congo, said that nine people (as opposed to 58) died in the Congo this year. This official also said there were 465 (as opposed to 1,284) confirmed cases in the nation, but did not specify the time period during which these cases occurred.
Possibly a clerical error explains the discrepancy, but we could not confirm this.
Alongo explained the persistence of the disease: “The residents enter the forest, pick up the corpses of monkeys, bats, and rodents which are the reservoirs of monkeypox.”
In any case, this form of the disease is rarely mentioned. If you go to the World Health Organization website and click on the question “Can people die from monkeypox,” you will find this unqualified statement:
Around 3–6 percent of reported cases have led to death in endemic countries [country of origin] in recent times, often in children or persons who may have other health conditions. It is important to note that this may be an overestimate because surveillance in endemic countries is limited.
Why don’t they point out that, if surveillance is limited, then those figures could also be an underestimate, rather than an “overestimate”? Not that I believe that is the case, but it’s an obvious possibility, surely worth mentioning.
Also, as explained above, that low death rate, “around 3-6 percent … in endemic countries,” only refers to west African countries — not the Congo Basin countries, where a more virulent form of the disease is thriving, and where over 10 percent have died of it.
The Congo does business with many non-African countries. What if this more dangerous form spreads to the rest of the world?
How the Disease Progresses
The Centers for Disease Control and Prevention (CDC) on the course of the disease:
Signs and symptoms usually occur 7 to 14 days after exposure to the virus and begin with a fever, headache, muscle aches, and exhaustion. One to three days after a fever starts, patients develop a rash that usually begins on the face and then spreads to other parts of the body, resulting in lesions that typically last for two to four weeks.
And, according to the WHO, swollen lymph nodes, sore throat, and coughing are additional symptoms.
In the majority of recent cases in Europe, young men had lesions on their genitals. But it’s not considered a sexually transmitted disease because it’s not spread through semen or vaginal fluids. So condoms wouldn’t prevent it.
People become infectious once the symptoms begin. But the first symptoms are common to many diseases, including influenza. Notice how that distinctive rash comes last… so there may be nothing to warn you — before the appearance of the rash — that the person you have been with is infectious.
Will It Mutate?
It’s comforting to know that monkeypox mutates slowly. One reason is that it’s a DNA virus, which is more stable than an RNA virus, like COVID-19. Here’s more, from FactCheck.org:
Based on the limited number of monkeypox viral sequences that scientists have analyzed so far, all of the outbreak viruses are virtually identical but differ from their closest known relatives, which were responsible for outbreaks in 2018 and 2019, by around 50 nucleotides.
That’s more than would be expected, since monkeypox viruses mutate quite slowly, with only about one or two changes per year.
As Trevor Bedford, a computational biologist studying viral evolution at the Fred Hutchinson Cancer Center, said on Twitter, the “~47 mutations suggest at least [the] potential” for there to be a “genetic component that would facilitate human-to-human transmission of the current outbreak viruses.” Still, he said, it was “unclear.”
Bravo, Trevor Bedford, for saying the potential for monkeypox mutating was “unclear.”


