
Veterinarians in Crisis
Veterinary hospitals are being stretched to their limits by the impact of COVID-19.
In June, Jasper, a 3-year-old border collie mix, tussled with a stand of foxtail grass. When his human, Heather, realized that a foxtail awn — the plant’s barbed, bristly seed head — was lodged in his nose, she knew it was important to seek medical care immediately. If not removed quickly, foxtails can lead to infections and abscesses and may even migrate to the brain, where they can cause more damage and even death.
Heather called the dog’s usual general practice veterinary hospital, but the next appointment was at least a month out. This was her first indication that she and Jasper would be reckoning with the seismic shift which has taken place in veterinary medicine over the past year and a half. She called emergency vet hospitals, and each had estimated wait times from six to 10 hours. After she and Jasper sat in the parking lot of an emergency hospital for seven hours, the dog was finally treated and then discharged around 2 a.m. While they waited, fortunately, the suspected foxtail irritation began to resolve; the alternative might have been fatal.
This is only one example of the difficulties veterinary medicine practices are encountering as the pandemic persists. Faced with the pressure to maintain coronavirus-era sanitation and safety regulations, as well as the expectation to provide timely animal health care, many clinics and hospitals are making unusual adjustments to operate at even a fraction of pre-pandemic efficiency. Despite these efforts, the needs of patients and their human owners are largely unmet.
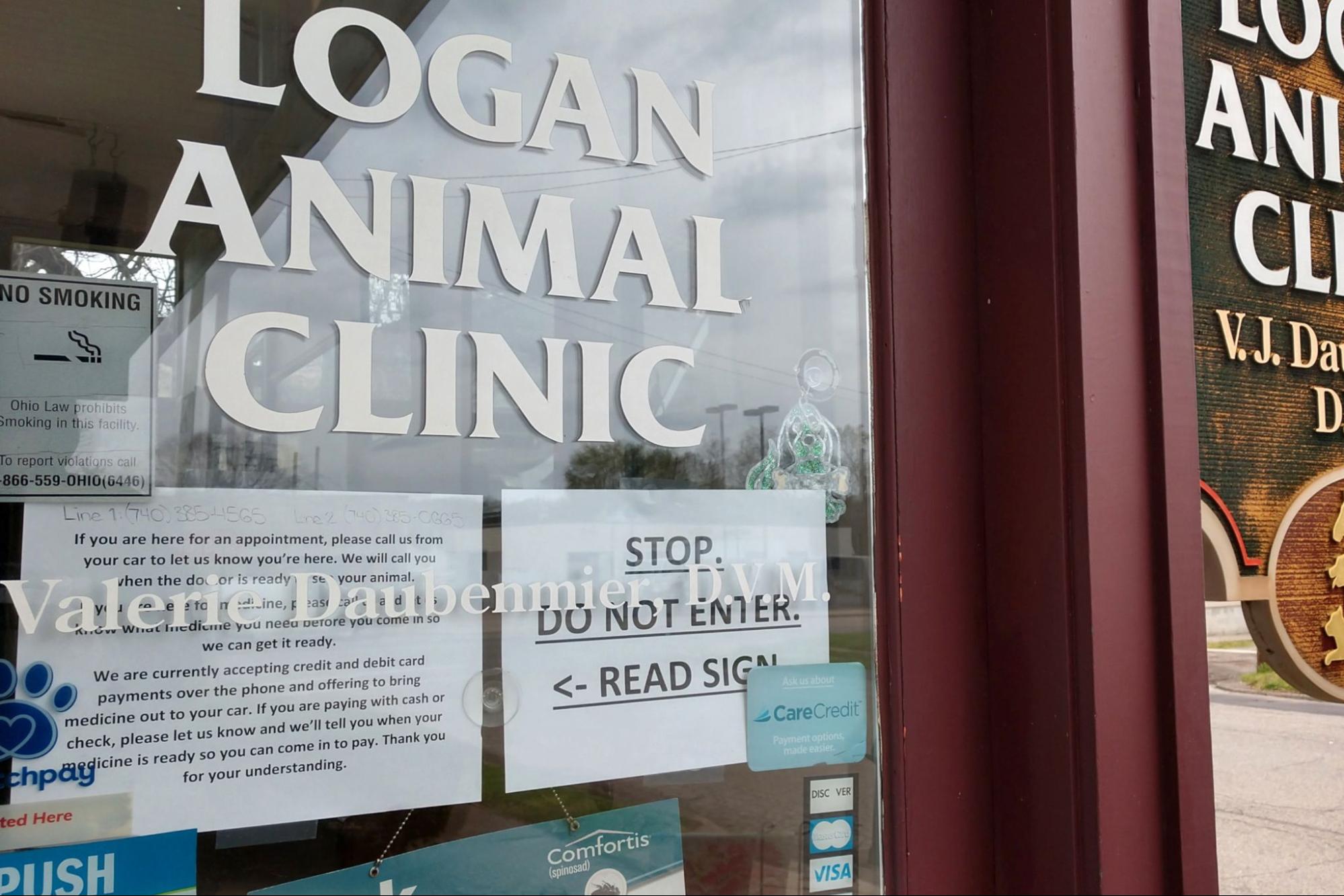
Countless apologies fly across waiting rooms, through phone lines, and are taped onto clinic windows in exasperated announcements. Dozens of owners are turned away at the door after four, six, even eight hours of anxiety-punctuated waiting.
A shortage of veterinary technicians, the sudden and frequent onslaught of “max capacity” periods, and the boom of pet adoptions and stay-at-home employment are remaking the landscape of veterinary practice. Accounts from veterinarians practicing during this tumultuous time reveal just how dire the situation has gotten.
Short on Staff and on a Short Leash
“Priority level restriction (PLR),” “pause,” and “max capacity” are just a few of the terms to describe the sudden implementation of hospital shutdowns for pandemic safety. A fully functioning veterinary hospital can go from running at high volume and efficiency to completely closing its doors to new patients within moments of reaching maximum capacity.
These restrictions are implemented to ensure patient and staff safety when the hospital is unable to take in any new patients. During pandemic operations, housekeeping has increased to include regular cleaning of public spaces and extra time for veterinary technicians to change their personal protective equipment (PPE) (a practice that may vary depending on the stress put on hospital capacity and state of limited resources).
The cause of these limitations on clinic operations is the shortage of vet techs. According to Sam Fahmi, a customer service representative at a veterinary hospital in Los Angeles, many doctors could not practice without the assistance of the techs on shift, who were often occupied with other appointments or delayed by stricter housekeeping measures. Kate Maynard, a veterinarian practicing in San Francisco, notes some of the many reasons clinics became short-handed: “[Since] unemployment plus a stipend may actually pay more than some technicians [or] receptionists make working, many support staff have quit. Or, because of the overwhelming patient load, many are calling out sick from the stress. Being short-staffed adds to the extended wait times.”
Seeking early and preventative health care — the standard and goal of veterinary practice under normal circumstances — becomes impossible when hospitals are short staffed and at max capacity. Owners are turned away at the door if their pets are not in critical condition. Cases that would have been admitted, like chronic lameness, gastrointestinal issues, or irregular coughing and sneezing, as well as more serious issues in their early stages (a foxtail irritation, foreign body ingestion, lack of appetite, infections, or fractures, for example), are turned away. As a result, when cases become dire enough to warrant admittance, treatment is often more expensive, intensive, and less likely to have a positive outcome.
To put numbers to this new reality, Maynard estimates: “Per shift I used to have approximately 5-10 inpatients, see 7-10 emergency walk-ins and have a wait time of an hour at most. Now I have 13-17 inpatients, up to 30 walk-ins, and 4-8 hour wait times.”
A State of General Emergency
Even when an animal is in critical condition, their admission to a veterinary hospital is not guaranteed, nor is it likely to be timely. Fahmi recounts the repeated and heartbreaking onslaught of devastated owners carrying dying dogs to the hospital, finally getting an appointment where the only remaining treatment option is euthanasia.
Worse still, the meaningful pre-pandemic euthanasia procedures — where you could hold your pet’s paw during the process, for example — are now characterized by a detached efficiency and absent farewells. Under suspended operations, clinics may refuse clients entry even when their pets may be admitted. Fahmi described the distress that filled her clinic when it was forced to refuse entry to a mentally unstable client alongside his admitted dog. For some owners, especially those whose pets are emotional support companions, this separation poses risks for both the owner’s mental health and the safety of the veterinary staff who must communicate and enforce regulations.
Another pandemic-era stress on general practice (GP) veterinary hospitals comes from the extra time many owners are now spending with their pets, as well as the surge of new owners during the pandemic. According to Maynard, “Puppies are not being appropriately vaccinated, spayed/neutered, or socialized. This has led to an increase in life-threatening preventable infectious diseases, unwanted pregnancies, and behavioral issues.” As a result, vet hospitals are ill-equipped to handle the greater volume of cases. To put numbers to this new reality, Maynard estimates: “Per shift I used to have approximately 5-10 inpatients, see 7-10 emergency walk-ins and have a wait time of an hour at most. Now I have 13-17 inpatients, up to 30 walk-ins, and 4-8 hour wait times.”
Adding additional stress, according to an emergency room (ER) veterinary doctor practicing in the greater Chicago area, is the increase in the types of cases being seen in the ER. This shift is in large part due to the bottleneck in short-staffed GP hospitals at max capacity. With these hospitals booked out weeks in advance, extra, “non-emergency emergency” cases are funneled into the ER, maxing out its capacity for real emergency cases. Maynard notes, “ERs are now full of these non-urgent patients who could not get into their GPs, as well as all these new sick, pregnant, or injured puppies. … ER wait times are astronomically longer and actual urgent patients are having to wait while a simple ear infection is taking up the doctor and staff’s time.” In Massachusetts, another veterinarian recounts how GP and emergency clinics alike were unable to support a cat with intensive care needs, resulting in its untimely euthanasia.
Impatience and Inpatients
Some changes wrought on veterinary practice by the pandemic, though, are positive. For one, the development of curbside care has increased the efficiency of patient drop off and pick up. Without having to meet pet owners, veterinarians have found more freedom to multitask while monitoring patients and speaking to owners over the phone. Pandemic-era visitation limitations have also inspired clinics to pick up digital tools, such as this vet-to-client mobile app where staff can send videos and photos to update owners on their pets’ statuses.
The veterinary system is in need of relief and assistance to address its newfound burdens and recently exacerbated old plights such as low pay and burnout. The few improvements to veterinary practice brought about by the pandemic cannot obscure the extra stress and dangers it has put upon the system. Maynard describes the hardest hitting changes effected by the pandemic:
The increase in the sheer number of angry owners as well as the ferocity of the abuse, I believe, are the most detrimental effects of the pandemic. People have become cruel… Career-damaging, defamation-of-character Yelp reviews have never been worse, nor have they been more inaccurate and unfair. And quite frankly, we have neither the time nor the energy to rebut them, which only adds to the feeling of helplessness felt by so many vets right now.
Not only has verbal abuse become the norm, but actual violence has escalated. In the last year my hospital has had our doors broken through multiple times by owners barging in, windows smashed, and death threats. People have lost their damn minds.
I love my job. I love improving and saving the lives of helpless, voiceless animals. I love relieving the stress, fear, and sorrow of an owner who would do anything for their beloved pet. I could not imagine doing anything different. But this truly is a toxic love-hate relationship, most predominantly because of abuse by owners. And the pain inflicted on veterinarians and veterinary staff has reached code red status.
So respect your vet and vet staff. Be accountable for your pet’s care. Be patient. Be kind. Be grateful. Wear the damn mask. Just be better so we can all get through this together.



{kind=link}