
The War on Opioids has created some unintended victims: Patients with chronic pain who no longer receive the help they needed… sometimes with deadly consequences.
|
Listen To This Story
 |
Rebecca’s* (name changed to maintain her confidentiality) life of chronic pain started at age 13. In a rollover car accident, she sustained a fractured hip, a dislocated and fractured femur, and another fracture that shattered the front of her pelvis into two separate pieces. After various complications and spending three months in the hospital, oscillating between intensive care, surgeries, and bedrest, she was finally released with plates and screws in her pelvis. For the most part, Rebecca returned to a normal life, until her back and hip pain reemerged about 15 years later.
This time, misdiagnoses, another set of surgeries, and steroid medications failed to treat her pain. Various physicians and surgeons — including those at world-renowned medical facilities — said that there was nothing more they could do to treat Rebecca’s condition. She also tried a number of alternative therapies, all to no avail.
At age 28, Rebecca began to see a pain management doctor, a step that is often viewed as a last resort, who prescribed her opioid medications.
“The first time the doctor took over my case, he literally gasped in horror at the state of my SI [sacroiliac] joint and back and was like ‘Oh my gosh, I didn’t realize how bad everything was until I saw the X-ray in-person,’” Rebecca told WhoWhatWhy.
After several weeks of agony, with the medication she was finally able to sleep for more than a couple of hours a night, return to her full-time job in public accounting, and have a life outside of her pain.
Yet a lot has changed since then. Rebecca is now 51 years old, and her pain has worsened with age and degeneration.
At the same time, as a byproduct of the opioid epidemic, doctors have grown more reluctant to prescribe narcotics.
“Every time I go in, he [my doctor] sees what’s going on. … Even though my pain is much worse than it was when I first started taking the medications, I’m only given enough medication to give me eight hours of relief in any 24-hour period,” Rebecca said.
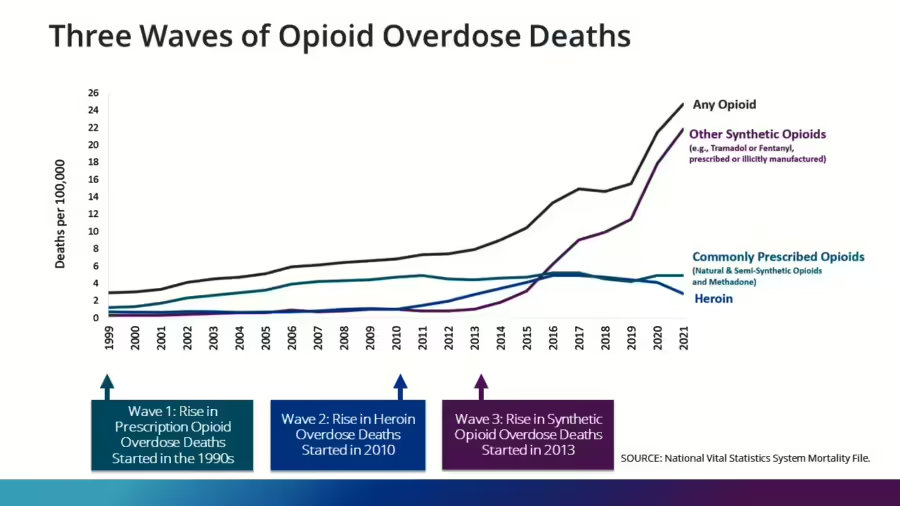
She is one of many pain patients who view themselves as collateral damage in the fight against the opioid epidemic, which has killed over 700,000 Americans since 1999. Prescription opioids were a significant culprit in the crisis, causing nearly 300,000 deaths, and fueling the “first wave,” between 1999 and 2011.
However, the Centers for Disease Control and Prevention (CDC) has found that since 2017, deaths due to prescription opioids have decreased annually, and that “commonly prescribed opioids are no longer driving the overdose epidemic.”
The second wave of the epidemic, which began around 2010, was driven by heroin. And in 2024, the United States is in its third and fourth waves of the epidemic. Overdose deaths are now driven by synthetic opioids, particularly illegally made fentanyl, as well as the increased use of multiple illegal substances simultaneously, like fentanyl in combination with psychostimulants like methamphetamines and cocaine.

The DEA vs. Doctors: A Climate of Distrust and Fear
Rebecca has asked her doctor about increasing her medication, to which he responds with concerns about being targeted by federal agencies.
“He says, ‘Look, I’m already writing this dose, and I’m concerned about the CDC and DEA [Drug Enforcement Administration] coming after me. Despite all the documentation you have and the therapies you’ve done, I’m just too afraid of losing my license,’” she stated.
Her doctor declined to be interviewed, citing concerns over CDC and DEA officials who “can shut down a doctor’s practice without evidence of wrongdoing even if they are following the guidelines from the CDC.”
Dr. Richard Kirkpatrick, owner and physician at a family practice clinic in Longview, WA, discussed this fear among prescribers in his clinic, following national news stories of doctors who were prosecuted for prescribing opioids to chronic pain patients. His clinic currently manages around 500 of these patients, and it initially started only about 50 of them on opioid treatment.
“The other doctors are willing to help a little bit [in treating chronic pain patients with opioids], but they don’t want to have primary responsibility,” Kirkpatrick said. “Two of the four physician assistants won’t write [opioid] prescriptions. They won’t even write a temporary prescription to cover somebody when things happen. … Because they’re afraid of losing their licenses.”
The National Pain Advocacy Center, a policy-focused advocacy group of scientists, clinicians, and civil rights advocates, states that over 50 percent of doctors refuse to see patients who manage pain using opioids, and 81 percent are reluctant to.
And doctors may be reluctant for good reason. Alongside pharmaceutical companies and other entities, overprescribing physicians have been held to blame for instigating the opioid epidemic.
In the late 1990s, a liberalizing culture in medicine around the treatment of pain, fraudulent marketing that certain opioids were nonaddictive, and physicians criminally prescribing opioids for their personal profit (“pill mills”) drove the overprescribing that led to the opioid epidemic.
While increased scrutiny of physicians’ prescribing practices may have helped diminish inappropriate prescriptions of opioids, the DEA has also targeted doctors who might have been prescribing opioids appropriately.
“As the population of doctors willing to receive those patients shrinks, whoever does receive them either has to stop [prescribing] opioids or risks looking like an outlier,” Kertesz described. Moreover, states like California have medical boards that have initiated investigations of doctors who prescribe opioids, based on such “outlier” principles.
One prominent and consequential example of this was the DEA’s suspension of Dr. David Bockoff’s ability to prescribe controlled substances in 2022. Bockoff was a Beverly Hills-based pain management physician who served many chronic pain patients.
As of 2024, he has not faced any criminal charges, according to Kristen Ogden, a patient advocate involved in legal action on behalf of Bockoff against the DEA. After his suspension, two of his patients died: one by suicide due to inadequate pain management (according to his suicide note), and another from complications related to opioid withdrawal and existing medical conditions.
Louis Ogden, Kristen Ogden’s husband and a former Bockoff patient with a rare genetic illness, was previously under the care of Dr. Forest Tennant, an addictionist and internist based in West Covina, CA.
Tennant “retired in 2018 under pressure from the DEA, although he was never even charged with anything at all,” Kristen said.
Tennant corroborated this, adding, “The DEA came in and looked at the records, and that pretty soon set them [the DEA] back, because they realized all my patients were dying.” He decided to shut down his clinic due to fear of being at risk of lawsuits, which are more likely to happen after such investigations, he explained.
The DEA’s investigations of a doctor can have radiating impacts, reducing the willingness of other doctors in that community to prescribe opioids, leading to the abandonment of pain patients.
Kate Nicholson, the executive director of National Pain Advocacy Center and a civil rights attorney, shared her own story of pain with WhoWhatWhy.
As a result of a surgical injury to spinal nerves, she was receiving care for her pain in Colorado, when a local, “well-respected” doctor fell under investigation by the DEA. This resulted in her own doctor deciding it was too risky to continue prescribing opioids.
“It just sent shockwaves through the whole community,” she said. “I went into the doctor’s office one day, and my doctor said, ‘You know, I’m not going to prescribe opioids to any of my patients anymore. Effective immediately.’ And I’m just having my first chance in two decades to learn to walk again. I was really afraid that it would undermine my progress.”
A 2022 study in West Virginia more broadly confirms these dynamics, finding that legislation intended to reduce inappropriate opioid prescribing resulted in physician fear of disciplinary action. In turn, this contributed to forced tapering and under-prescribing of opioids, as well as the notion that “taking on patients who legitimately required opioids could jeopardize their career.”
‘Bureaucratic and Institutional Momentum’ From a Bygone Era
In 2016, as part of an effort to combat the unfolding opioid crisis, the CDC issued its initial Opioid Prescribing Guidelines, which included rigid dose limits. Following the issuance of these guidelines, many patients were being forced off of opioids that they were benefitting from and functioning well with, leading to adverse mental health outcomes including suicide, studies showed.
As a result, the CDC issued updated guidelines in 2022 to be more flexible and individualized. It repudiated the 2016 dose limit, directing physicians to exercise caution when prescribing opioids but also acknowledging the harms of forcing patients off of opioids.
However, the CDC’s updated guidelines in 2022 might have been too little and too late to change the pervasive and generalizing anti-opioid atmosphere.
Dr. Stefan Kertesz, University of Alabama-Birmingham physician and researcher, explained that “bureaucratic and institutional momentum” following the 2016 guidelines has led to many insurance and Medicaid programs to retain strict dose limits.
“Even though the CDC has entirely repudiated this dose limit, it’s being enforced in my own state’s Alabama Medicaid program,” said Kertesz.
The revised CDC guidelines will take time to truly penetrate the medical field, experts believe. Ameliorating doctors’ fears of prosecution and changing narratives in medicine and society around prescription opioids are part of what is needed to restore opioid access for patients who need them.
Outside of the evolution of CDC guidelines, a fundamental change in the nature of the opioid crisis also leaves a stringent focus on prescription opioids outdated.
Since the opioid epidemic is now driven by synthetic opioids, continued momentum of targeting prescription opioids may no longer serve to effectively combat today’s opioid epidemic, while causing collateral damage: the pain patients whose lives depend on opioid treatment
Kirkpatrick, the Washington-based family practice physician, said that in his state, a very low percentage of overdose deaths are due to prescription opioids. The state’s Department of Health website shows that as of 2023, 10 percent of overdose deaths are related to prescription opioids, a percentage that appears to have been steadily falling since at least 2019.
At the same time, the 2023 data shows that 78 percent of overdose deaths were caused by illicitly manufactured fentanyl, 67 percent caused by any stimulant, and 51 percent caused by both an opioid and a stimulant. This data fits into the characterizations of the third and fourth waves of the opioid epidemic.
However, targeting prescription opioids could help mitigate the fentanyl crisis. Fentanyl overdose deaths often occur when the drug is sold as ‘heroin,’ affecting those who transitioned from prescription opioids to heroin during the second wave of the opioid epidemic. By reducing dependence on prescription opioids, experts say we may decrease demand for heroin, ultimately lowering fatalities linked to fentanyl.
The ‘Outlier’ Principle: A Rudimentary Numbers Game
Litigation that has helped keep pharmacies and distributors accountable for their role in the opioid crisis creates additional pressures against the prescription and distribution of opioids, leaving patients unable to access medication.
Kertesz explained that the National Opioid Settlement requires drug distributors to avoid shipping opioids to “outlier” pharmacies, those that exceed an expectation for the amount of opioids they should be releasing. Under pressure from distributors, pharmacies have an incentive to profile “outlier” prescribers, and stop honoring their prescriptions.
While, to Kirkpatrick’s knowledge, his clinic has never been investigated by the DEA or state medical boards regarding opioid prescriptions, various pharmacies announced that they were no longer going to honor his clinic’s prescriptions. According to Kirkpatrick, the pharmacy chains usually stated that his clinic was ordering “inappropriately high doses of narcotics.”
Kirkpatrick wrote back to the pharmacies and the Pharmacy Quality Assurance Commission, informing them of the flexibility and nuance around opioid prescribing in the CDC’s 2022 guidelines. He received no response to any of his letters, and he believes the pharmacies’ refusal to honor his clinic’s prescriptions is an attempt to avoid fines related to the National Opioid Settlement.
While such profiling of outliers may have helped shut down pharmacies and prescribers who were associated with “pill mills,” distributing millions more opioids than their communities could possibly need, they also pressure doctors legally prescribing necessary opioids to avoid taking on pain patients or to force existing patients off opioids.
“As the population of doctors willing to receive those patients shrinks, whoever does receive them either has to stop [prescribing] opioids or risks looking like an outlier,” Kertesz described.
Moreover, states like California have medical boards that have initiated investigations of doctors who prescribe opioids, based on such “outlier” principles.
“I have periodically come across cases where it appears that parties associated with the medical board simply investigate whoever has high-dose patients, inviting witnesses to review the charts,” Kertesz said. “They argue — very simplistically — that a patient’s unexpected behavior, [like] using illicit drugs or not showing up for an appointment, is a sign that a doctor’s prescription is potentially criminal.”
The “outlier” principle of identifying potentially wrongdoing doctors is an example of the ‘bounded rationality’ of public policies, he added. The number of opioid prescriptions a doctor writes is only a rough, sweeping heuristic in identifying suspect doctors: While it might effectively target inappropriately overprescribing doctors, it might also take aim at innocent doctors who simply more often treat pain patients who require opioid medications.
The hesitancy of doctors to serve chronic pain patients who require opioids is reflected in patient experiences. Rebecca called 15 to 20 doctors before she found one who would take her, following the retirement of her previous doctors. Nicholson and the Ogdens had to travel thousands of miles to find a doctor who would prescribe opioids for their pain. Following Bockoff’s suspension, Danny Elliott, a former patient of Bockoff, and his wife called 17 doctors, all of whom refused to take Elliott on as a patient. Elliott and his wife died by suicide shortly after, due to the despair around his untreated pain.
* * *
For Rebecca, this state of affairs spells a life of awaiting misery and — more often — living in it.
“With the amount of medication I’m given for a 30-day period, it often means that I get no more than one to two hours of sleep a night,” she said. “I’m up at night sobbing in pain, there’s nothing I can do about it. I mean, I’m using ice packs, heat pads, TENS units [electrical nerve stimulation devices used to relieve pain], everything you can think of, and nothing is helping.”
Her pain prohibits her from being present in the most significant aspects of her life: She cannot work full-time, and her ability to be present for her husband, daughter, and family events — like her daughter’s orchestra concerts — is scarce.
“That’s why this year, I got a DNR [a “do-not-resuscitate” order] put in place,” she explained. “I will not actively commit suicide — I don’t want to do that to my daughter or my husband. But if I were to get in a car accident tomorrow, I would absolutely refuse any kind of life saving care, because my quality of life is so poor. It’s like, why would I want to keep doing what I’m doing right now?”
Perhaps the worst part of Rebecca’s experience of untreated pain is the loneliness of it all.
“Not many people want to hear about it,” she said. “My husband and best friends know, but they don’t want to hear every day that I’m in pain. It is a lonely existence, and it’s also a miserable existence. And a lot of people do not understand.”


